Ready to take the next step?
Find out which treatment fits your health best.
Get startedNo commitment until clinician review
Cancel anytime




.webp)
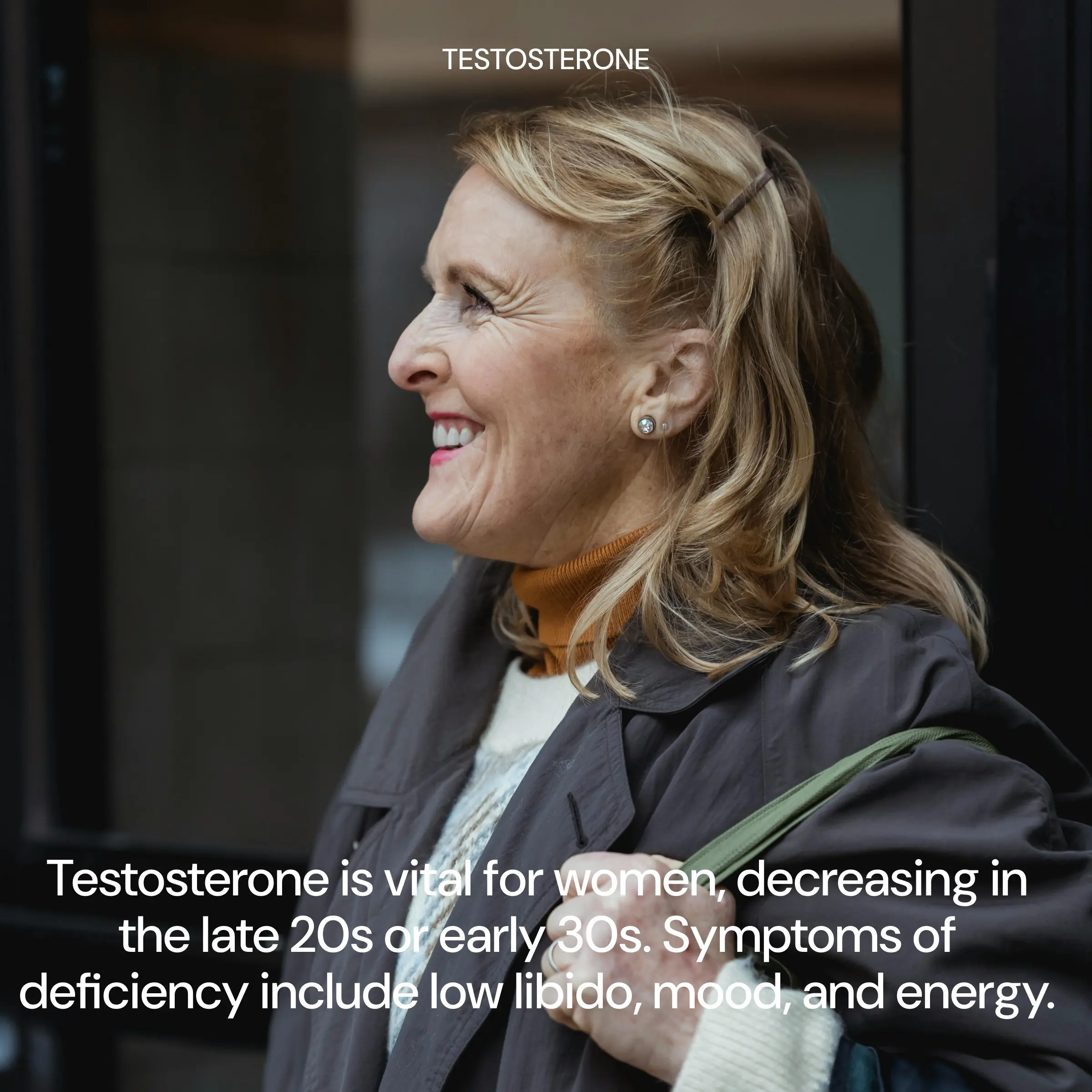
Testosterone isn’t just a “men’s hormone.” Women make it too, and levels can decline with age, surgical menopause, or hormonal shifts. For some postmenopausal women, that drop is linked to persistent low sexual desire with distress (often called HSDD), even after addressing common contributors like vaginal dryness, sleep, stress, mood, medications, and relationship factors.
Get startedTestosterone – systemic androgen therapy designed to deliver steady, low-dose testosterone through the skin. Clinical best practice is to maintain female physiologic blood levels, not “high” or “performance” dosing.
Because testosterone products are often formulated for men, women’s therapy requires individualized dosing and careful titration. If prescribed, your clinician will:
Side effects are more likely if testosterone levels rise above the physiologic female range. Possible effects include:
Testosterone Gel is a prescription hormone therapy used in menopause care primarily for postmenopausal women diagnosed with HSDD (low sexual desire that causes personal distress) after a biopsychosocial assessment. Current consensus statements emphasize that this is the only evidence-based indication for testosterone therapy in women.

Images are for illustrative purposes only. Individual results may vary. Compounded medications are not FDA-approved.
Desire is multi-factorial—hormones are only one piece. When testosterone is truly low and other contributors are addressed, restoring testosterone to the physiologic female range may help support the neurobiological pathways involved in sexual interest and responsiveness. In clinical studies of transdermal testosterone for HSDD, women experienced improvements in desire and reduced distress compared with placebo.
Images are for illustrative purposes only. Individual results may vary. Compounded medications are not FDA-approved.
Testosterone gel is applied to clean, dry skin and allowed to fully dry. Because topical testosterone can transfer via skin contact, safety steps matter: wash hands after applying, cover the application site with clothing once dry, and wash the site before skin-to-skin contact.

Images are for illustrative purposes only. Individual results may vary. Compounded medications are not FDA-approved.


Testosterone gel is a prescription, topical form of testosterone applied to the skin. For some women in peri-/menopause, it may be used to support symptoms linked to low androgen levels, most commonly low libido, low energy, and reduced sense of well-being.
Many women prefer gel because it’s non-invasive and easy to use at home. It can also offer steadier day-to-day dosing. The best option depends on your symptoms, lab values, and what fits your routine.
Testosterone therapy is most often considered for low sexual desire, reduced arousal, low energy, decreased motivation, and difficulty maintaining strength. Results vary, and treatment should be guided by both symptoms and lab monitoring.
Some women notice subtle changes in energy or mood within a few weeks. Libido and performance-related changes often take longer. Many clinicians reassess around 6–12 weeks to evaluate response and adjust dosing if needed.
You’ll apply it exactly as prescribed (usually once daily) onto clean, dry skin. The most important part is consistency: apply at the same time each day and follow your clinician’s instructions on placement and amount.
Yes, skin-to-skin transfer is possible until the gel fully dries and the area is covered. Let it dry completely, wash your hands after applying, and follow guidance on clothing coverage and timing before close contact.
Yes. Baseline labs help confirm whether testosterone is appropriate and guide safe dosing. Follow-up labs help ensure your levels stay in a healthy range for women and reduce the risk of side effects.
Not necessarily. In appropriate doses, testosterone may support strength and body composition for some women. However, hormones can influence appetite, water retention, sleep, and energy, so your plan should include monitoring and lifestyle support.
Side effects are often dose-related and may include acne, oily skin, increased facial/body hair, scalp hair thinning (in those predisposed), and mood or sleep changes. If side effects appear, your clinician can adjust your dose.
These effects are uncommon at carefully managed, female-appropriate dosing, but they can occur if levels run too high. Report early signs (voice changes, increased hair growth, clitoral sensitivity changes) promptly so your clinician can reassess.
Often, yes. Many menopause plans include estrogen and progesterone, and testosterone may be added when appropriate. Your clinician will tailor the combination based on symptoms, labs, and medical history.
Testosterone may not be appropriate if you’re pregnant or breastfeeding, have certain hormone-sensitive conditions, or have uncontrolled medical issues that require stabilization first. Your clinician will review your history and help choose the safest option.м

If your understanding of hormone replacement therapy is shaped by headlines from 20 years ago, it’s time for an update. The 2002 Women’s Health Initiative (WHI) study sent shockwaves through medicine, leading millions of women to abandon HRT and a generation of physicians to stop prescribing it. But the decades since have brought dramatic clarity: the WHI’s findings were widely misinterpreted, and the resulting fear of HRT caused immeasurable harm to women who could have benefited from treatment.
Today, major medical organizations including the North American Menopause Society, the Endocrine Society, and the American College of Obstetricians and Gynecologists affirm that HRT is safe and effective for most women experiencing menopause symptoms, particularly when started within 10 years of menopause onset.
Luvo’s hormone replacement program is built on this modern evidence base. With 10 medication options spanning estradiol formulations, testosterone therapy, and non-hormonal alternatives, it offers a level of treatment personalization that most competitors simply can’t match.
Menopause isn’t a single event — it’s a transition that typically spans several years. The process begins in perimenopause, usually in the mid-40s, when the ovaries begin producing less estrogen and progesterone. Hormone levels fluctuate unpredictably, causing symptoms that can range from mildly annoying to severely disruptive.
Menopause is officially reached when 12 consecutive months pass without a menstrual period, typically around age 51. At this point, the ovaries have largely ceased producing estrogen, and levels of this hormone remain permanently low.
Estrogen isn’t just a reproductive hormone. It has receptors throughout the body — in the brain, bones, cardiovascular system, urogenital tract, skin, and joints. When estrogen declines, the effects cascade across multiple systems: vasomotor symptoms like hot flashes and night sweats, sleep disruption, mood changes and cognitive fog, vaginal dryness and urogenital atrophy, bone density loss, cardiovascular risk changes, joint pain and muscle loss, and skin and hair changes.
Testosterone also declines in women, though more gradually. By menopause, a woman’s testosterone level may be half what it was in her 20s, contributing to decreased libido, reduced energy, and loss of muscle mass.
HRT addresses these declines by restoring hormones to levels that alleviate symptoms and protect long-term health.
What sets Luvo apart from competitors is the breadth of our medication options. Managing hormonal decline isn’t one-size-fits-all, and neither is our program.
Estradiol is available in five formulations: oral tablets for systemic hormone delivery, transdermal cream for absorption through the skin, transdermal patches for steady-state hormone levels, vaginal gel for localized urogenital symptom relief, and vaginal tablets for targeted vaginal atrophy treatment.
Testosterone for women is available in three formulations: injection, oral tablets, and topical gel — addressing the often-overlooked role of testosterone in female vitality, libido, and body composition.
Non-hormonal options include Paroxetine, the only FDA-approved non-hormonal treatment for vasomotor symptoms, and Desvenlafaxine, an SNRI with strong evidence for hot flash reduction. These serve women who cannot or prefer not to use hormonal therapy.
This 10-medication toolkit means your Luvo provider can design a protocol precisely matched to your symptoms, health history, preferences, and risk profile.
HRT is most clearly indicated for women experiencing moderate to severe vasomotor symptoms such as hot flashes and night sweats, women under 60 or within 10 years of menopause onset (the “window of opportunity” for cardiovascular and bone benefits), women with premature ovarian insufficiency or early menopause (before age 40), women with significant urogenital symptoms like vaginal dryness, painful intercourse, or recurrent UTIs, and women at elevated risk for osteoporosis.
HRT may require additional evaluation or alternatives for women with a history of breast cancer, women with active cardiovascular disease or a history of blood clots, women with undiagnosed vaginal bleeding, and women with active liver disease.
Luvo’s providers conduct thorough health evaluations to determine the safest and most effective approach for each patient. For women who cannot use estrogen, our non-hormonal options provide meaningful symptom relief.
Explore Luvo’s full hormone replacement program to learn more.
The Women’s Health Initiative (WHI) study, published in 2002, is the most influential — and most misunderstood — study in the history of hormone replacement therapy. Its initial results, which were widely reported as showing that HRT causes breast cancer and heart disease, led to millions of women abruptly stopping treatment and a generation of providers becoming afraid to prescribe it.
The human cost of this overreaction has been enormous. Women suffered through severe menopause symptoms unnecessarily. Rates of osteoporotic fractures increased. The gap between what the evidence actually shows and what many women (and some providers) believe about HRT remains one of the biggest failures of medical communication in modern history.
This article provides a clear, evidence-based assessment of what we actually know about HRT safety in 2026.
The WHI studied two specific regimens: oral conjugated equine estrogens (Premarin) plus medroxyprogesterone acetate (Provera) in women with a uterus, and Premarin alone in women who’d had a hysterectomy.
The estrogen-only arm actually showed a decreased risk of breast cancer and no increased cardiovascular risk. It was stopped early simply because it was part of the same administrative trial as the combination arm.
The combination arm showed a small increased risk of breast cancer (8 additional cases per 10,000 women per year) and a small increased risk of cardiovascular events. However, these risks were concentrated in women who started HRT more than 10 years after menopause and were over age 60 — a population very different from the typical woman who begins HRT in her early 50s.
Critically, the WHI used oral conjugated equine estrogens (derived from horse urine, containing multiple estrogen compounds) and a synthetic progestin (medroxyprogesterone acetate) — not the bioidentical estradiol and micronized progesterone that modern HRT typically uses. Subsequent research has shown that bioidentical formulations and transdermal delivery have substantially different risk profiles.
Breast cancer risk with modern HRT is more nuanced than headlines suggest. Estrogen-only therapy does not increase breast cancer risk and may reduce it. The combination of estrogen plus micronized progesterone (the bioidentical progestogen) appears to carry less breast cancer risk than the synthetic progestins used in the WHI. When risk does exist, it’s small in absolute terms and similar to risks associated with common lifestyle factors like alcohol consumption, obesity, and sedentary behavior.
Cardiovascular risk depends heavily on timing. The “timing hypothesis” is now well-established: women who start HRT within 10 years of menopause or before age 60 show neutral or even beneficial cardiovascular effects. Women who start HRT later may face increased risk. This window of opportunity is a key consideration in Luvo’s prescribing approach.
Venous thromboembolism (blood clot) risk is increased with oral estrogen but not with transdermal estrogen. This is one of the most clinically actionable findings in modern HRT research — and it’s why Luvo offers transdermal options (cream and patches) alongside tablets.
Stroke risk shows a similar pattern to clotting risk: modestly increased with oral estrogen, not increased with transdermal delivery, and dose-dependent. Using the lowest effective dose and transdermal delivery minimizes this concern.
Luvo’s hormone replacement program is designed with risk minimization built into every level.
Formulation selection matters. Luvo uses bioidentical estradiol, not conjugated equine estrogens. The availability of transdermal options (cream and patches) allows women with clotting risk factors to avoid oral estrogen entirely.
Route-of-delivery matching means your provider recommends the delivery method based on your risk profile, not just convenience. Women with elevated thrombotic risk are guided toward transdermal options. Women with predominantly vaginal symptoms may use localized therapy with minimal systemic exposure.
Non-hormonal alternatives ensure that women who cannot safely use estrogen still have effective treatment options. Paroxetine and Desvenlafaxine provide meaningful relief without any hormonal exposure.
Timing considerations are respected. Luvo’s providers follow the evidence-based window of opportunity, recommending HRT initiation for appropriate candidates within 10 years of menopause onset.
Ongoing monitoring through regular follow-ups ensures that treatment remains appropriate and effective over time, with dose adjustments as needed.
This comprehensive, evidence-informed approach to risk management is what distinguishes Luvo from competitors that offer a limited menu of options with minimal clinical nuance. Explore the full hormone replacement program.

Of all the symptoms of menopause, vaginal and urogenital changes may be the most underreported and undertreated. Up to 80% of postmenopausal women experience genitourinary syndrome of menopause (GSM) — a term that encompasses vaginal dryness, burning, irritation, painful intercourse (dyspareunia), urinary urgency and frequency, and recurrent urinary tract infections.
Unlike hot flashes, which often improve over time, GSM is progressive. Without treatment, it gets worse with each passing year as the estrogen-dependent tissues of the vagina and urinary tract continue to thin, lose elasticity, and become increasingly fragile.
The good news: localized vaginal estradiol is one of the most effective, safest, and most well-tolerated treatments in all of HRT. Luvo offers two vaginal estradiol formulations — vaginal gel and vaginal tablets — specifically for this purpose.
GSM occurs because the vaginal and urethral tissues are highly estrogen-dependent. When estrogen levels drop during and after menopause, these tissues undergo significant changes.
The vaginal epithelium thins from multiple cell layers to just a few, becoming fragile and easily irritated. Vaginal pH rises from its normal acidic range (3.5–4.5) to neutral or alkaline levels, disrupting the protective microbial environment and increasing susceptibility to infections. Blood flow to the vaginal and urethral tissues decreases, reducing natural lubrication and tissue health. The vaginal walls lose elasticity and may actually narrow and shorten. The urethral lining thins, contributing to urinary symptoms.
These changes can profoundly affect quality of life and intimate relationships. Many women avoid sexual activity entirely because of pain, and urinary symptoms can restrict daily activities. Yet studies consistently show that fewer than 25% of affected women receive treatment — often because they don’t mention symptoms to their provider, or their provider doesn’t ask.
Vaginal estradiol delivers the hormone directly to the tissues that need it most. Unlike systemic estradiol (tablets, cream, or patches), vaginal formulations are designed for localized action with minimal absorption into the bloodstream.
When applied vaginally, estradiol is absorbed by the estrogen-receptor-rich cells of the vaginal epithelium. It stimulates cell proliferation and maturation, restoring the vaginal lining to a healthier, more resilient state. Vaginal pH normalizes, protective lactobacilli return, lubrication improves, and the tissue regains elasticity and blood flow.
The systemic absorption of vaginal estradiol is very low — significantly lower than oral or transdermal estradiol. Blood estradiol levels with vaginal formulations typically remain within the normal postmenopausal range. This is why vaginal estradiol is considered safe for many women who cannot use systemic HRT, including some breast cancer survivors (though this should always be discussed with an oncologist).
Luvo offers two formulations for localized estradiol delivery.
Estradiol vaginal gel is applied intravaginally using a pre-measured applicator. The gel distributes evenly across the vaginal walls, providing broad tissue contact. Many women find the gel comfortable and easy to use. Application is typically daily for the initial treatment period, then reduced to a maintenance schedule of 2–3 times per week. The gel formulation can also provide some benefit to the external vulvar area during application.
Estradiol vaginal tablets are small tablets inserted into the vagina using a disposable applicator. They dissolve and release estradiol locally. The tablet format is clean, mess-free, and appeals to women who prefer a solid formulation over a gel. Like the gel, initial treatment is usually daily, transitioning to a maintenance schedule.
Both formulations are effective for treating vaginal dryness, painful intercourse, vaginal atrophy, and urinary symptoms. The choice between them often comes down to personal preference and comfort.
Explore Luvo’s estradiol vaginal gel and estradiol vaginal tablets.
Understanding whether you need localized therapy, systemic therapy, or both is an important conversation to have with your Luvo provider.
Vaginal estradiol alone is appropriate if your primary symptoms are urogenital — vaginal dryness, painful sex, urinary issues — and you don’t have significant hot flashes, sleep disruption, or other systemic symptoms. It’s also a good option for women who have contraindications to systemic estrogen or prefer to avoid it.
Systemic estradiol (tablets, cream, or patches) is needed if you have systemic symptoms like hot flashes, night sweats, mood changes, or bone density concerns. Systemic therapy also provides some benefit to vaginal tissues, though many women find that adding localized vaginal estradiol provides more complete urogenital relief.
Combination therapy — systemic plus vaginal — is appropriate for women who have both systemic and significant urogenital symptoms. The systemic dose is set for overall symptom management, while vaginal estradiol provides the concentrated local effect the vaginal tissues need.
Luvo’s program supports all three approaches, and your provider will recommend the strategy that best addresses your symptom profile. Visit the hormone replacement program page to get started.

.webp)







